

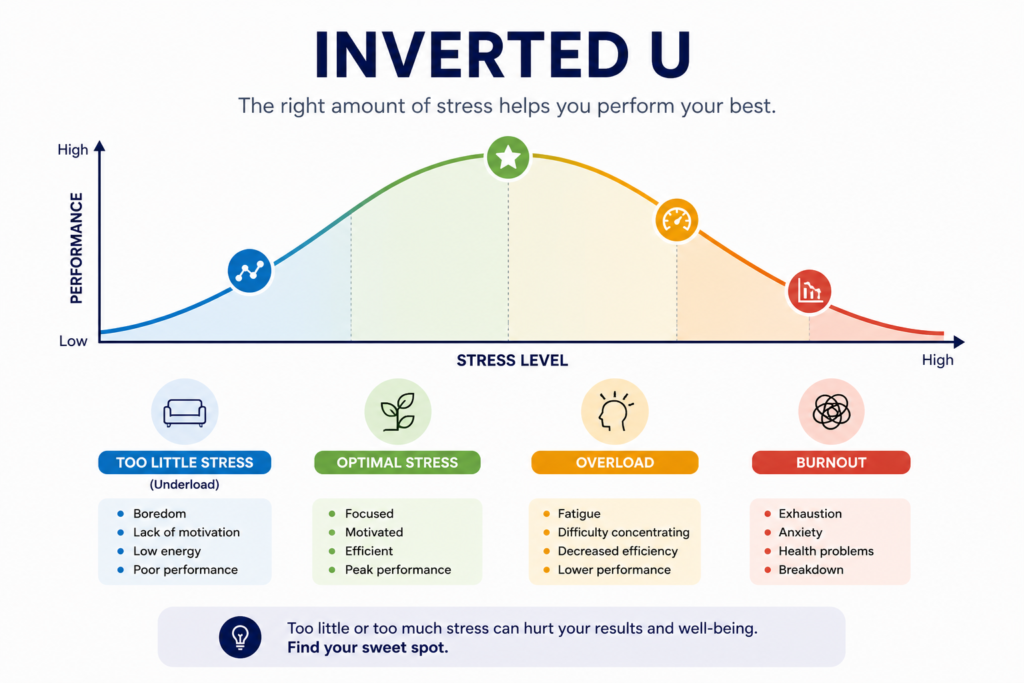
The inverted U is one of the most useful mental models you can carry into clinical practice and leadership. Most people understand it as the Yerkes-Dodson curve: performance rises as pressure increases, peaks, then falls. But the deeper idea is broader than stress and arousal. It applies to almost anything where you assume more is better, or less is safer. At a certain point, the thing that was helping starts hurting. The dose becomes the poison. The intervention becomes the harm.
Malcolm Gladwell explored this in David and Goliath with class sizes and parenting styles. The same curve kept appearing: smaller classes improve outcomes, until the class is so small that peer learning disappears. More money improves child outcomes, until parents can no longer say no to anything. The pattern is the same. And primary care is full of it.
With my geriatric interest, the first place i’ve noticed this was with frail patients.
1. Glycaemic Control in Frail Older Adults
This is probably the clearest clinical example in general practice right now.
Tighter HbA1c reduces microvascular complications. That is real. But once you push into the 48-53 range in a frail 84-year-old on three hypoglycaemic agents, you start generating more harm than you prevent. Hypoglycaemic episodes, falls, fractured neck of femur, hospitalisation. The ACCORD trial had to be stopped early because intensive glycaemic control in high-risk patients increased mortality.
The fix for most of these patients is not optimisation. It is de-intensification. But the system, and often the patient, has been conditioned to believe that lower is better.
Let’s look at another example from the frailty cohort.
2. Blood Pressure Management and Frailty
A systolic of 120 mmHg used to look like a win. The SPRINT trial showed tight control reduced cardiovascular events.
But apply the same logic to a frail 78-year-old with postural hypotension, and you get a different outcome entirely. Syncope. Falls. AKI from relative hypoperfusion. Hypertension in the Very Elderly Trial (HYVET) showed that treating hypertension in adults over 80 produces real benefit. But its population was selected. The most frail, those already falling, already dependent, already living on reduced physiological reserve, were not well represented. Apply those same targets to that patient, and you are no longer on the rising arm of the curve.
You will have patients on your list right now who are over-treated on antihypertensives. Their BP looks controlled on paper. Their QOF entry is clean. And they are at increased risk of a fall because their systolic drops to 90 when they stand up.
3. Appointment Access and Continuity
This one plays out in almost every practice.
Open access improves same-day availability. That sounds straightforwardly good. But push it far enough and you destroy continuity. Patients cannot book with their named GP. Long-term conditions drift. Relationships dissolve. The care that requires someone to know the patient over time, frailty management, complex multimorbidity, safeguarding, becomes fragmented.
On the other side, practices that tried to preserve continuity at the expense of access during and after COVID ended up with appointment waits that drove patients to urgent care centres and A&E, or delayed presentations of serious pathology.
The peak is a blend. Named GP, proactive care for the complex patients, combined with enough access capacity that acute presentations do not back up. Neither extreme works. Both feel logical when you are only looking at one side of the curve.
4. Patient Empowerment and Information-Giving
Shared decision making is the right clinical approach. Informed consent is the right ethical standard. But there is an inverted U here too.
A patient who receives nothing and is just told what to do cannot participate meaningfully in their care. A patient who is handed an 18-page decision aid about statins after a 10-minute consultation is often more anxious and less decided than when they walked in. There is research on this: decision fatigue and information overload can reduce the quality of patient choices, not improve them.
The skill is calibrating the amount of information to the patient’s health literacy, their current emotional state, and the complexity of the decision. More information is not always more empowered.

5. GP Workload and Performance
This is a personal one, and it is probably familiar.
There is a version of you as a clinician where you are stretched enough that you are engaged, growing, solving real problems. You are making decisions, managing relationships, running the practice alongside your clinical sessions, and you feel the productive edge of pressure. That is the peak of the curve.
Then something tips. A partner or colleague leaves. A CQC inspection lands. The GP trainee has a struggling placement and needs more of your time. The PCN director role lands in your lap. Each one feels manageable alone. Stacked, they push you past the peak.
When that pressure has been building long enough, your decision quality drops before you notice it. You start avoiding the hard conversations because you do not have the bandwidth to manage the aftermath. You start rubber-stamping things rather than interrogating them. That is not laziness. That is what happens when you are operating on the descending arm of the curve.
The fix is not just resilience training or another wellbeing webinar. It is recognising where the peak is and protecting your position relative to it. That means knowing what to stop as clearly as you know what to start.
That is the practical value of this model. It gives you a framework to act on, not just reflect on.
The Practical Takeaway
The inverted U is not a reason to do less. It is a reason to ask where the peak is for the specific thing you are dealing with, in the specific patient or system you are working with. The dangerous assumption is that the relationship between input and output is linear, that more treatment means more benefit, more access means better care, more clinical sessions means more productivity. In reality, the curve bends. It always bends.
Your job, as a clinician and in your personal life, is to find the peak and to know when you are past it.
Read more about How To Bounce Back From Stress.

